Home
There are multiple factors and barriers that lead to inequities surrounding female permanent contraception, or sterilization. This site is dedicated to the research by Dr. Kavita Shah Arora and team regarding the clinical disparities, public health impact, ethical complexities, and need for policy reform.
Background
Half of all women who request postpartum permanent contraception do not undergo their desired surgery after delivery or in the postpartum period. As many as half of these women become pregnant within the following year.
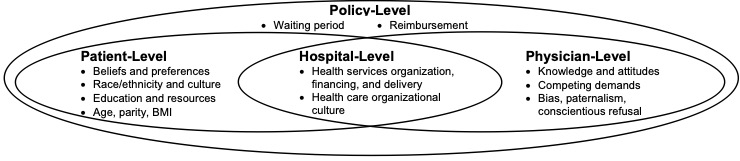
There are many drivers leading to inequitable postpartum permanent contraception. These include factors at the patient-level as well as barriers at the clinician-, hospital-, and policy-levels. At the patient level, differences in knowledge surrounding contraceptive options as well as partner/familial/cultural context regarding contraceptive preferences shape contraceptive decision-making. At the clinician level, implicit biases and competing clinical demands impact contraceptive counseling and provision. At the hospital level, decisions regarding OR prioritization and availability, staffing, and reimbursement impact permanent contraception fulfillment. Finally, at the policy level, the federal Medicaid sterilization policy, which mandates a specific consent form and waiting period, is a known barrier to care. This policy was established due to coerced sterilizations on women of color and low socioeconomic status. Today, women with Medicaid are half as likely to obtain a desired postpartum sterilization as those with private insurance. Compounding this disparity, women of color with Medicaid are less likely to achieve sterilization fulfillment compared to white women with Medicaid.
Recent Publications
Ongoing contraceptive goals of patients who did not achieve desired postpartum permanent contraception prior to hospital discharge
Viswanathan et al., Contraception, 2024
Modeling the impact of decreasing waiting period length for Medicaid sterilization: A multi-site cohort study
Berg et al., Contraception, 2024
Fulfillment of Permanent Contraception among Patients with Cesarean Delivery in a Multi-Site Cohort
Bullington et al., Maternal and Child Health Journal, 2024

Documentation of prenatal contraceptive counseling and fulfillment of permanent contraception: a retrospective cohort study
Viswanathan et al., Reproductive Health, 2024
Medicaid and Fulfillment of Postpartum Permanent Contraception Requests
Arora et al., Obstet Gynecol, 2023
